What is red light therapy?
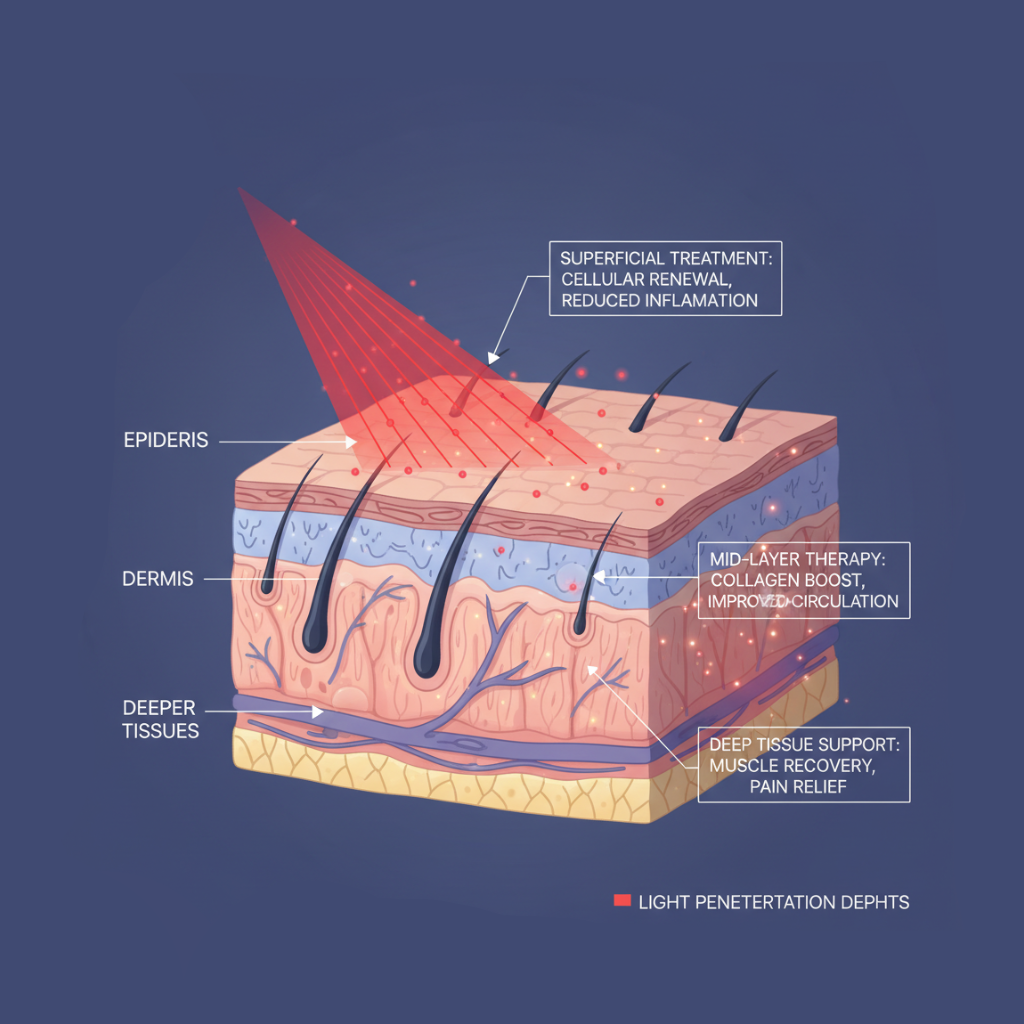
Red Light Therapy (RLT) is a non-invasive treatment that uses low-level red or near-infrared light at specific wavelengths (typically 600–900 nm) to irradiate body tissues and produce therapeutic effects. This treatment modulates cellular function through photochemical reactions.
How Does Red Light Therapy Work at the Cellular Level?
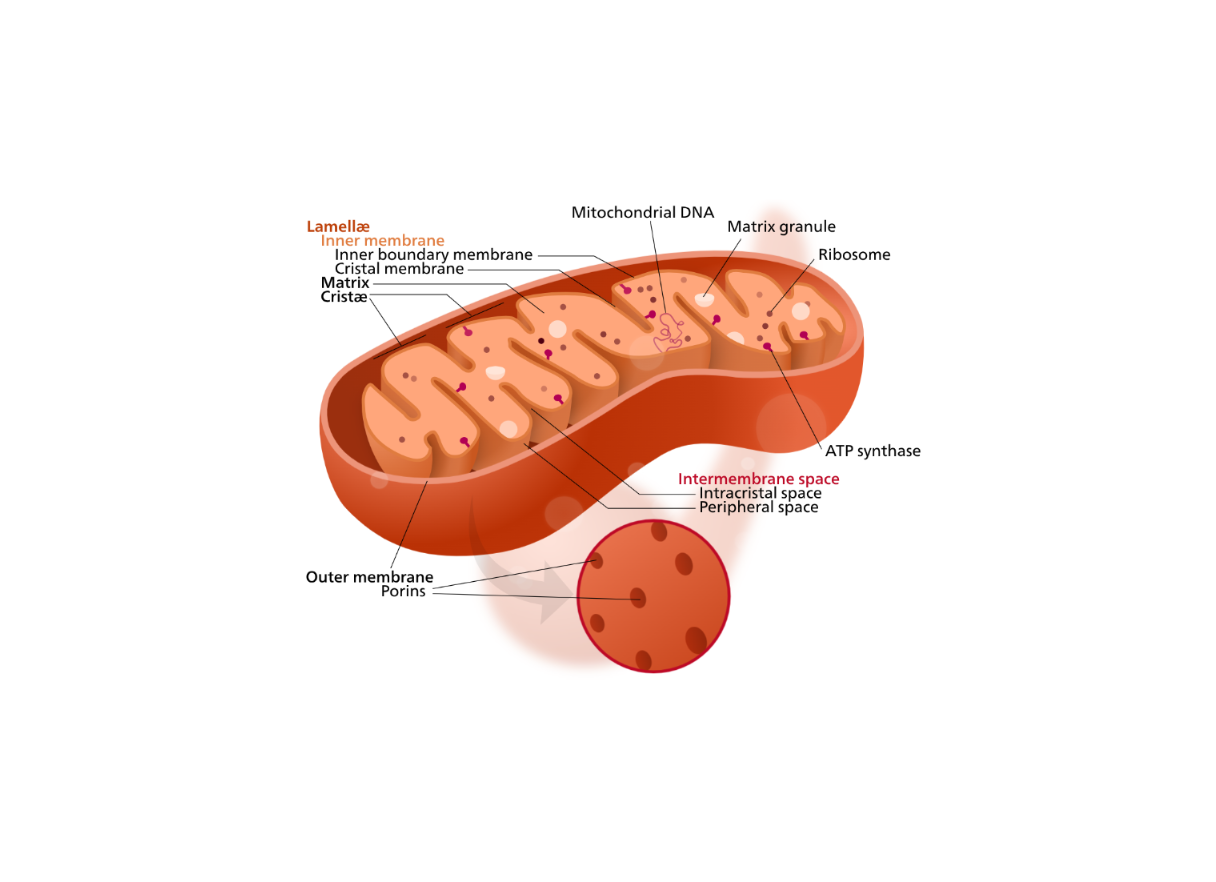
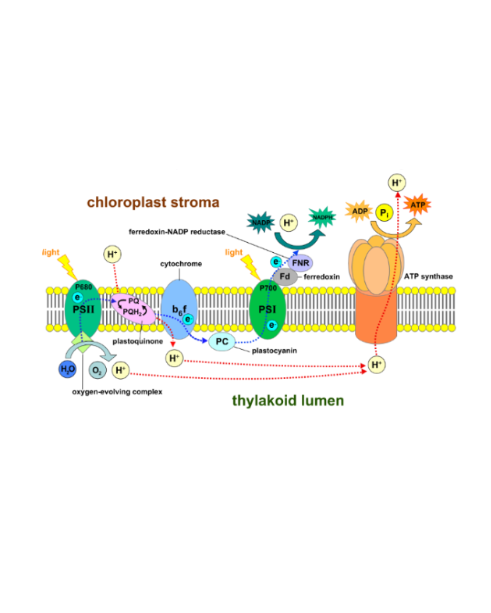
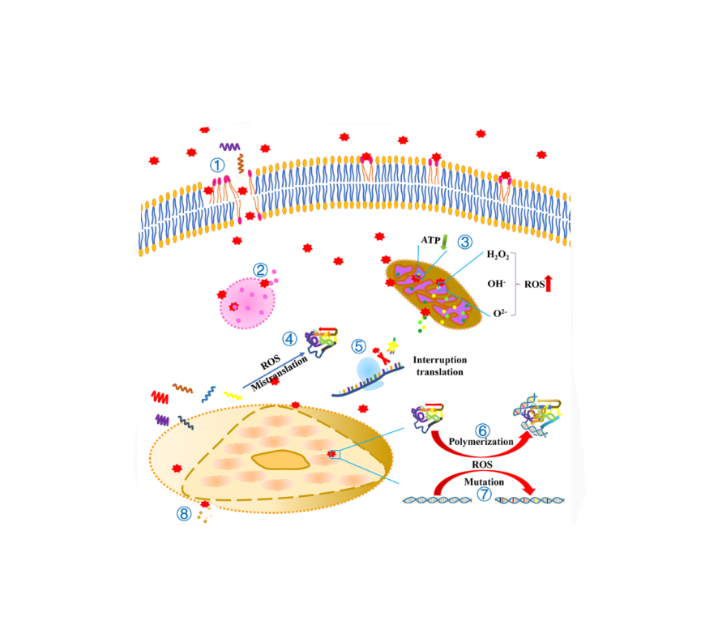
The mechanism of red light therapy is based on the absorption of photons by Cytochrome c Oxidase (CCO) in the mitochondria. When light of a specific wavelength is absorbed, it stimulates the production of adenosine triphosphate (ATP), reduces oxidative stress, and regulates reactive oxygen species (ROS) levels. These changes ultimately lead to altered gene expression, increased cell proliferation, and anti-inflammatory effects.
Studies have shown that red light therapy can enhance cellular metabolism, promote collagen synthesis, and improve local microcirculation.